
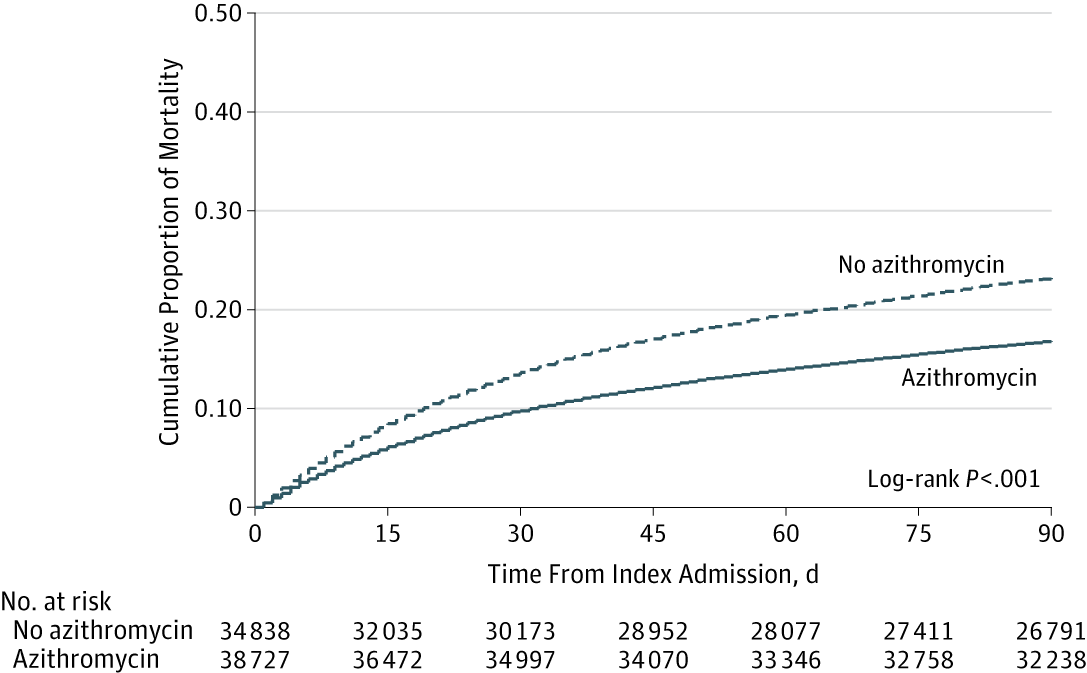
 Cochranized in the past, macrolides (usually azithromycin) seem more convincingly beneficial regarding mortality and treatment failure in pneumonia (especially in the elderly). This large but retrospective VA registry analysis supports this suggestion. The finding of more MIs but fewer ‘cardiac events’ is confusing. First line for everyone, include it in the initial antimicrobials, continue it despite negative atypical screen, avoid in ischaemic heart disease – I don’t think we know yet.
Cochranized in the past, macrolides (usually azithromycin) seem more convincingly beneficial regarding mortality and treatment failure in pneumonia (especially in the elderly). This large but retrospective VA registry analysis supports this suggestion. The finding of more MIs but fewer ‘cardiac events’ is confusing. First line for everyone, include it in the initial antimicrobials, continue it despite negative atypical screen, avoid in ischaemic heart disease – I don’t think we know yet.
Macrolides still look good for pneumonia
Thrombolysis for which PE patients – time to decide?
 Chatterjee’s MA after the recent swathe of studies suggests using thrombolysis (full dose) in PE all-comers results in less mortality and fewer recurrences even though bleeding occurs much more frequently (NNH 18). Disability and quality of life might be revealing but is rarely reported (re bleeding but staying alive). If restricted to the under 65s then it’s safer. Time to make up your mind – particularly about the younger patients with signs of right heart compromise!
Chatterjee’s MA after the recent swathe of studies suggests using thrombolysis (full dose) in PE all-comers results in less mortality and fewer recurrences even though bleeding occurs much more frequently (NNH 18). Disability and quality of life might be revealing but is rarely reported (re bleeding but staying alive). If restricted to the under 65s then it’s safer. Time to make up your mind – particularly about the younger patients with signs of right heart compromise!
Degrees of death
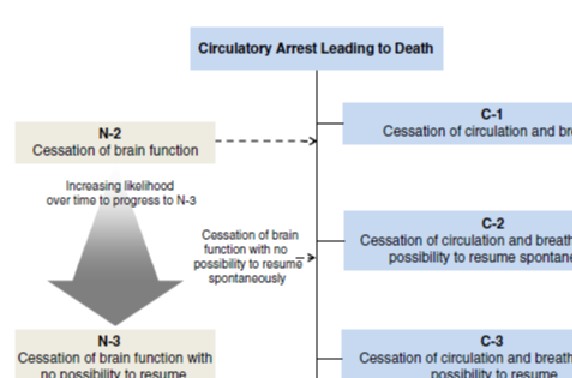 “Death is the permanent loss of capacity for consciousness and all brainstem functions”. C1-2 and N1-3 – the attempt to separate the often inseparable circulatory and neurological elements of dying and death. This guideline development provides a good glossary and some reassuring common sense in amongst some more complicated detail.
“Death is the permanent loss of capacity for consciousness and all brainstem functions”. C1-2 and N1-3 – the attempt to separate the often inseparable circulatory and neurological elements of dying and death. This guideline development provides a good glossary and some reassuring common sense in amongst some more complicated detail.
More on predicting outcome after TTM
 A multimodal approach is intuitively best but what’s the minimum you need to include in a predictive model? This small-but-nice study suggests clinical examination PLUS electroencephalography reactivity PLUS serum neuron-specific would give near certain forecast of a dreadful outcome.
A multimodal approach is intuitively best but what’s the minimum you need to include in a predictive model? This small-but-nice study suggests clinical examination PLUS electroencephalography reactivity PLUS serum neuron-specific would give near certain forecast of a dreadful outcome.
What honestly works for ARDS?
 If you ‘umbrellanalyse’ (my term, but you can use it) 20,000 patients with ARDS, it seems we’re not sure of much more than: DON’T oscillate, DO prone, and DO use low a Vt strategy. All else is futile?
If you ‘umbrellanalyse’ (my term, but you can use it) 20,000 patients with ARDS, it seems we’re not sure of much more than: DON’T oscillate, DO prone, and DO use low a Vt strategy. All else is futile?
Get adrenaline in early at non-shockable in-hospital arrests
 ‘Get with the guidelines’ latest registry analysis in the BMJ focusses on timing of adrenaline in non-shockable, in-hospital arrests. 12% of those given adrenaline at 1, 2 or 3 minutes survived to hospital discharge compared with 7% at 6 mins. Of note only 7% or 25,000 survived with favourable neurological outcome (moderate disability or better). Good Medscape analysis available.
‘Get with the guidelines’ latest registry analysis in the BMJ focusses on timing of adrenaline in non-shockable, in-hospital arrests. 12% of those given adrenaline at 1, 2 or 3 minutes survived to hospital discharge compared with 7% at 6 mins. Of note only 7% or 25,000 survived with favourable neurological outcome (moderate disability or better). Good Medscape analysis available.
ACEP epilepsy guidelines 2014
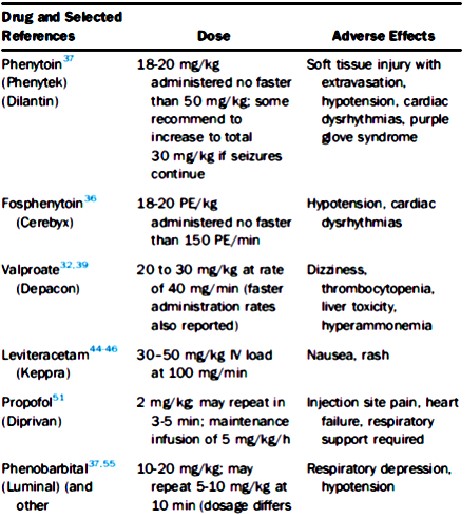 ACEP guidelines on epilepsy include a pragmatic section on status epilepticus. No drug clearly wins. Maybe stick to what you know. Benzodiazepine infusions probably best avoided?
ACEP guidelines on epilepsy include a pragmatic section on status epilepticus. No drug clearly wins. Maybe stick to what you know. Benzodiazepine infusions probably best avoided?
Probiotics to prevent C.diff diarrhoea: flawed evidence but Cochrane folk recommend it!
 A recent Cochrane review suggests probiotics (unspecified) reduce the incidence of C.diff diarrhoea (or symptomatic infection), but not C.diff infection per se. High heterogeneity, low quality of evidence, some counter-intuitive findings but somehow a moderate level recommendation that probiotics are good for patients on antibiotics. NB this was not an analysis of critically ill patients!
A recent Cochrane review suggests probiotics (unspecified) reduce the incidence of C.diff diarrhoea (or symptomatic infection), but not C.diff infection per se. High heterogeneity, low quality of evidence, some counter-intuitive findings but somehow a moderate level recommendation that probiotics are good for patients on antibiotics. NB this was not an analysis of critically ill patients!
 LITFL
LITFL
- Leonardo Gigli May 6, 2025
- Procedure: Serratus Anterior Block May 6, 2025
- Procedure: Serratus Anterior Block May 6, 2025
- Neuroimaging Cases 009 May 5, 2025
- Procedure: Lateral Canthotomy April 8, 2025
Wessex ICS BottomLine
- Clinical Decisions on Beta Blockers After MI April 23, 2025
- Critical Care Evidence Updates – March 2025 April 23, 2025
- Emergency Evidence Updates – March 2025 April 23, 2025
- NIV vs HFNC to prevent re-intubation in patients with obesity March 26, 2025
- Critical Care Evidence Updates – February 2025 March 21, 2025
St Emlyns
- Acute behavioural disturbances: olanzapine or haloperidol?
- Podcast – Social Media and Artifical Intelligence in Medicine with Peter Brindley at LTC
- Podcast – Monthly Round Up February 2025 – Skills Fade, Resuscitation Targets and more
- RCEM Conference 2025: Reflections from Day 3
- Life 2.0 – What the dead can teach us about living – Matt Morgan at TBS 2025
Emcrit
- EMCrit Wee – Neuroleptic Malignant Syndrome (NMS) Explosion May 1, 2025
- EMCrit Shadowboxing Case 9 – Spinal Cord Injury? April 24, 2025
- EMCrit 399 – Serotonin Syndrome (SS) and Neuroleptic Malignant Syndrome (NMS) – Primer Episode April 17, 2025
- 1:1 Nursing Podcast – Episode 0 – The Introduction April 15, 2025
- EMCrit 398 – NeuroEMCrit – NeuroMuscular Emergencies April 3, 2025
Thinking Critical Care
- A Cool Physiology Study on APRV-TCAV by Zou et al.: Our Thoughts! #FOAMed #FOAMcc
- Lionel Lamhaut’s Pre-Hospital ECMO course at HR25!!! May 24th and 25th, 2025!
- A Hemodynamic Rant with Korbin Haycock! #interfaces #FOAMed #FOAMcc
- Resus Chat with Matt Siuba! #FOAMed #interfaces #FOAMcc #FOAMer
- Interfaces with Rory Spiegel (@EMnerd)! #FOAMed, #FOAMcc, #FOAMer
Critical Care Northampton
- Low-dose clonidine infusion to improve sleep in postoperative patients in the high-dependency unit. A randomised placebo-controlled single-centre trial
- What about Rehab then….
- Frailty – a yes, or a no to ITU??
- Prolonged vs shorter awake prone positioning for COVID-19 patients with acute respiratory failure: a multicenter, randomised controlled trial
- Quick Draw Anatomy for Medical Students – Joanna Fox