
A guidance group and a sounding board of 50 UK experts has published guidelines on the management and ICU admission of critically ill adult patients with haematological malignancies. Part of the driving force for this was the ‘traditional nihilism’ in the critical care community about these patients, meaning disagreements regarding the benefit of admission to ICU are not uncommon (~15%).
Consequently this guideline is a mixture encouragement to be less pessimistic and a lot of reiteration of common sense. This is my rough summary and take on it.
Making the case
Data from small, retrospective, single centre studies in the 80’s and 90’s suggested a very poor outcome in leaukaemic patients requiring advanced organ support; up to 100% mortality if mechanical ventilation was used. As a result consensus by 2000 was that patients with haematological malignancy and metastatic solid organ tumours were not ‘good candidates’ for critical care admission.
However over subsequent years larger studies, mainly from databases, showed improving survival and suggested markers of poor prognosis (high APAHCE, vasopressor use, BM transplant, advanced age, and both disease and genetic subtypes). This is a result of improvements in chemotherapy, BMT preparation as well as supportive care.
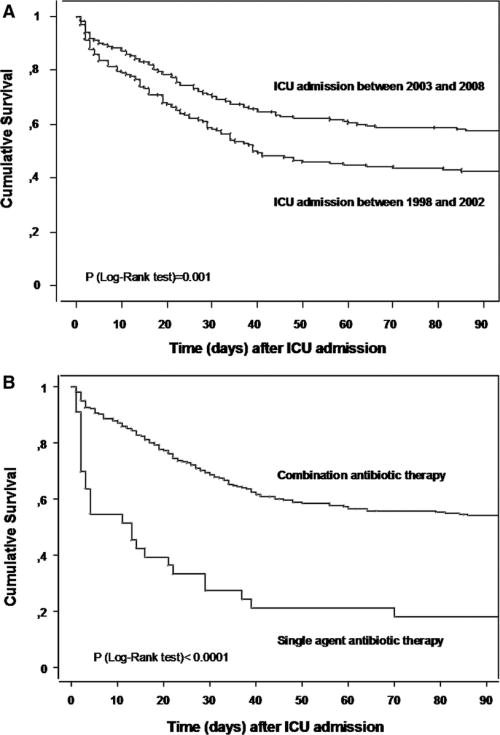
Mortality data from ICNARC published in 2009 revealed an ICU and hospital mortality of around 40% and 60% respectively.
Of note
- Sepsis and respiratory failure remain the most common reason for ICU involvement.
- Recent analysis suggests that older patients and those needing vasopressors do badly, and that dual antibiotic therapy (aminoglycoside + another) is protective. Survival rates had improved significantly over the course of the study.
- Patients who are admitted and are deteriorating after the first 3 days are likely to do badly, particularly those starting pressors or renal replacement after day 3.
- Even now, as with many of our patient groups, scores may predict how populations will do but none is accurate for your particular patient.
- The concept of a trial of ICU may be of value in these patients. Look for the more powerful prognostic markers on day 4/5 (MV, pressors and renal support).
- Aside from the standard considerations when making a decision to admit (premorbid state, prognosis, previous discussions re treatment limitations etc), remember to ask about:
- special transfusion requirements (e.g. irradiated products, cytomegalovirus (CMV)-screened)
- history of bleomycin exposure/radiotherapy
- isolation needs
Recommendations
- An aggregate track and trigger system should be in place to monitor patients. (1C)
- Surviving Sepsis campaign guidelines and NICE guidance on neutropoenic sepsis should be followed. (1C)
- ICU referral should involve direct discussion between an ICU consultant and a haematology consultant. (1D)
- Patients who are clearly in the process of dying with irreversible illness should not be referred to critical care. (1D)
- Survival is largely determined by the acute critical illness. Patients appropriate for further life-extending treatment or with good performance status should be considered for an unrestricted critical care ‘ICU Trial’. (1C)
- Use of non-invasive ventilation (NIV) in the ward for these patients is not advised. (1C)
- Patients who have undergone allogeneic haemopoietic stem cell transplantation (HSCT) should be transferred to an ICU attached to a level 3 British Committee for Standards in Haematology (BCSH) unit. (1D)
- Inter-hospital and intra-hospital transfer should follow the Intensive Care Society (ICS) 2011 Guidelines for the Transport of the Critically Ill Adult. (1C)
Much like the exposure of misplaced pessimism surrounding COPD patients in ICU a decade ago, we need to make sure our reluctance to admit adult patients with haematological malignancy to the unit is based on up-to-date outcome stats and opinions.
Which group next for pessimism busting? Metastatic solid organ tumours?
2 comments
Great post Justin, and well worth it.
Had a great chance to chat to James O’Beirne, a hepatologist at the Royal Free, about this concept for patients with advanced cirrhosis. https://itunes.apple.com/au/podcast/so-whos-bed-is-it-anyway-cirrhosis/id440626447?i=251744837&mt=2
We certainly do get a bit focussed on ‘putting up the wall’ sometimes without a great deal of evidence to support our assumptions. I think this is often done for the right reasons, but the execution is sometimes lacking.
Nice post
Author
Thanks Todd. Great podcast. My own ‘wall’ does seem to be getting weaker by the year. But I also find the trial of ICU is often not a clear cut manoeuvre and you’re left with someone who you know is very likely to do badly but isn’t deteriorating, making withdrawal difficult.