
Dabigatran is a direct thrombin inhibitor rapidly gaining popularity due to growing consensus that it is associated with less life-threatening bleeding than vitamin K antagonists. Measures to reverse the agent have a small evidence base and are limited to prothrombin complex concentrates, factor VIIa (less so) and haemodialysis/filtration (more so). The NIHR briefing from January summarizes near-current consensus.
A number of agents are currently being tested. 2 recent trials have looked at the most promising reversal agent, Idarucizumab, a monoclonal antibody fragment that irreversibly binds the drug.
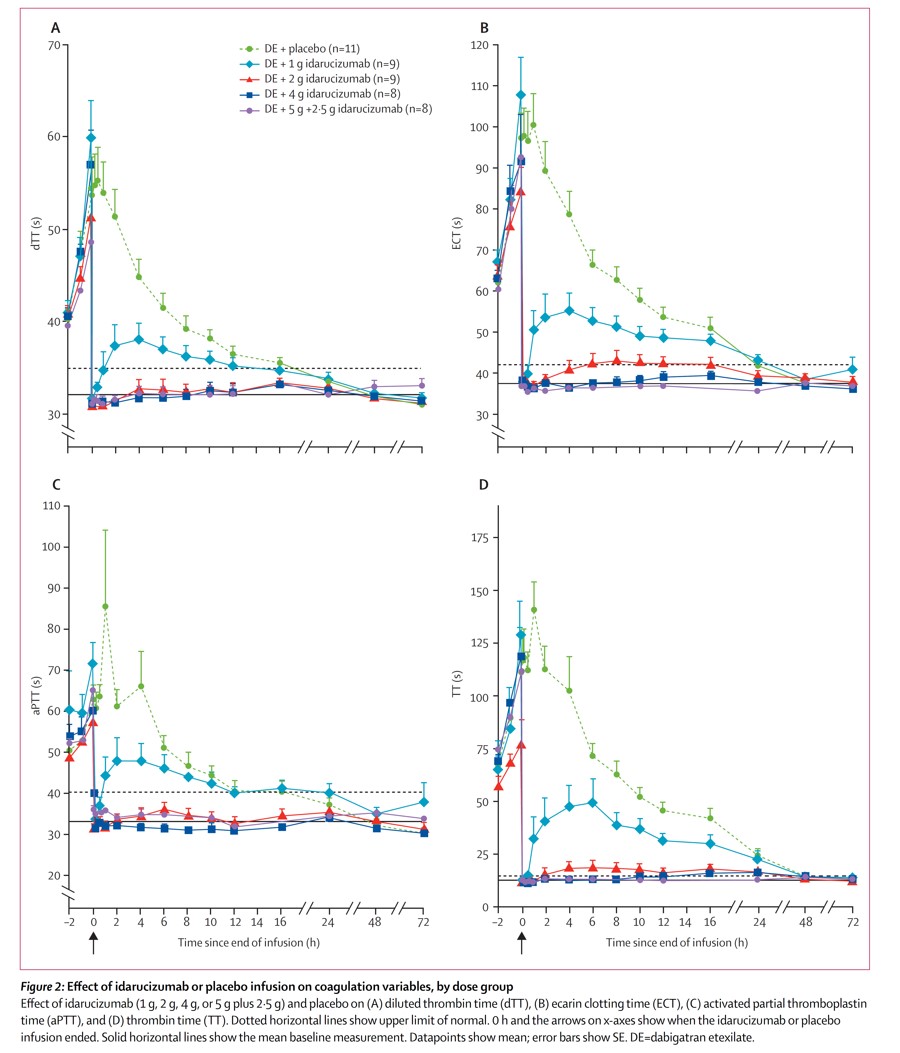
In the Lancet, a randomised, placebo-controlled, double-blind phase 1 trial of Idarucizumab also recently appeared.
Four groups of healthy males (47 in total) were given dabigatran for four days and then received either placebo or 1 g, 2 g, 4 g or 5g of idarucizumab two hours after the last dabigatran (peak plasma time)
All doses immediately reversed the dabigatran although the 1 g dose didn’t achieve a sustained effect.
Interestingly plasma concentrations of total dabigatran initially increased, but not its anticoagulation effect. This is presumed to be due to diffusion of unbound extravascular drug (idarucizumab has a low Vd) into the vascular space. Although Dabigatran-idarucizumab complex is excreted by the kidneys a recurrence of anticoagulation is not expected.
A thorough look-out for adverse events found nothing concerning
In the NEJM, RE-VERSE AD was prospective cohort study of the safety and efficacy of 5 g of idarucizumab in significant haemorrhage, or those requiring an urgent procedure. The primary endpoint was percentage reversal within 4 hours. The secondary end point was the restoration of haemostasis.
Dilute thrombin time and ecarin clotting time (recognized tests to monitor dabigatran levels) were normalized within minutes in the bleeding group. The median time to haemostasis was around 11 hours. In the group undergoing urgent procedures 33 of the 36 haemostasis during the procedure was sufficient.
There was only one episode of thrombosis, occurring 72 hours after the dose.
Of course, Idarucizmab won’t work for bleeding in the presence of factor Xa inhibitors (the ‘-Xabans’) for which the favoured treatment is Prothrombin Complex Concentrate. Parallel studies will hopefully offer encouraging results in the near future, for example, using Feiba.
So it looks good both in healthy volunteers and two small groups of patients. We await comparative studies and further safety data whilst managing these patients with our current ?suboptimal strategies. It may be infrequent that it’s really required but knowing it’s there would be reassuring!
(To impress on a ward round with your mastery of pronouncing awkward monoclonal antibodies, try “I dare you kiss Uma b”)
Other comment: