
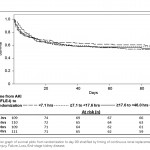
In this recent re-look at patients from a previous seminal study, a ‘nested’ cohort from the RENAL study with RIFLE ‘I’ acute kidney injury (GFR<50%, creatinine rise to twice baseline, UOP <0.5ml/kg for 12hr).were selected.
The APACHE III score for those supported late was significantly lower suggesting there may have been something different (a covariate, so not propensity matched) that added to confidence in delaying RRT.
Moreover only about 40% of those supported early had sepsis, against 60% of those receiving RRT after 48hr. This possibly reflects an element of faith in source control and circulatory support – give resuscitation a chance before firing up the filter. Presumably they were also less likely to be fluid overloaded, an indication for RRT know to carry poor outcome.
Urea level does not correlate well with time from start of AKI using RIFLE criteria. This is an issue that needs to be considered when looking at other studies on the same subject.
Acknowledging the dangers in concluding causality in observational studies, earlier RRT was not significantly associated with improved outcome but there was a suggestion of benefit (a trend towards mortality if delayed) that needs more exploring; large prospective studies in groups eg severe sepsis.
Do the dosing studies then need to be redone as well? An interesting single unit experience in saving money by switching to low volume (20ml/kg/hr) CVVHDF without changing clinical outcome was published this week.