Guidelines for the management of severe traumatic brain injury
Brain trauma foundation: 4th edition, 2016
This is a brief summary and some of the wording is changed for brevity, hopefully without too much loss of accuracy.
Although not explicitly stated on the guidelines, ‘Severe brain injury’ is generally defined as a brain injury resulting in a sustained [for a variable number hours] Glasgow Coma Scale of 3 to 8.
Also look at the recent RESCUEicp trial that’s referred to.
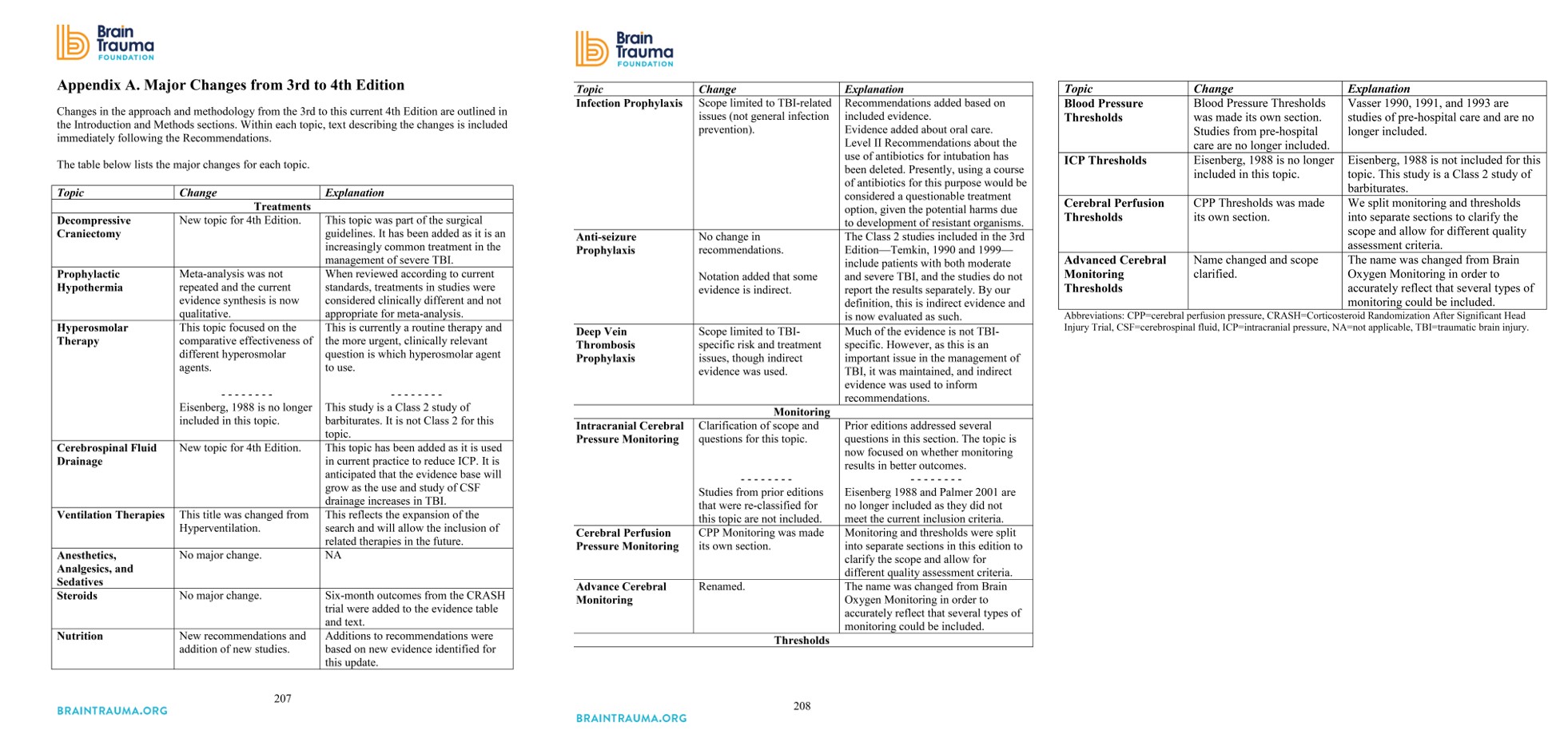
Decompressive craniectomy (DC)
Level II A only
- Bifrontal DC is not recommended in severe TBI with diffuse injury and ICP >20mmHg (for >15min in any hour). (re GOS at 6 months). May decrease ICU days.
- A large, rather than small, frontotemporoparietal DC is recommended severe TBI (better mortality and neurologic outcomes)
NB RESCUEicp trial may change this (checkout this video re DC).
Changes from Prior Edition
New topic.
Prophylactic hypothermia
Level II B only
- Early (within 2.5 hours), short-term (48 hours post-injury) prophylactic hypothermia is not recommended in diffuse injury.
Changes from Prior Edition
No change
Hyperosmolar therapy
Level I, II, and III
- May lower ICP but insufficient evidence on other outcomes.
Old recommendations not brought forward but restated (acknowledging complexity and evidence gaps):
- Consider Mannitol (0.25 g/kg to 1 g/kg) for ICP. Avoid arterial hypotension (systolic blood pressure <90 mm Hg).
- Restrict mannitol use prior to ICP monitoring to patients with signs of transtentorial herniation or progressive neurological deterioration not attributable to extracranial causes.
CSF Drainage
Level III
- An EVD system zeroed at the midbrain with continuous drainage of CSF may be considered to lower ICP burden more effectively than intermittent use.
- Use of CSF drainage to lower ICP in patients with an initial Glasgow Coma Scale (GCS) <6 during the first 12 hours after injury may be considered.
Changes from Prior Edition
New topic.
Ventilation
Level II B
- Prolonged prophylactic hyperventilation with partial pressure of carbon dioxide in arterial blood (PaCO2) of 25 mm Hg or less is not recommended.
Old recommendations, not brought forward, yet restated!
- Hyperventilation is recommended as a temporizing measure for the reduction of elevated ICP.
- Hyperventilation should be avoided during the first 24 hours after injury.
- If hyperventilation is used, use SjO2 or BtpO2 monitoring.
Anaesthetics, analgesics and sedatives
Level II B
- Administration of barbiturates to induce burst suppression measured by EEG as prophylaxis against the development of intracranial hypertension is not recommended.
- High-dose barbiturate administration is recommended to control elevated ICP refractory to maximum standard medical and surgical treatment. Hemodynamic stability is essential before and during barbiturate therapy.
- Although propofol improves ICP it doesn’t improve mortality or 6-month outcomes. Caution is required as high-dose propofol can produce significant morbidity.
Changes from Prior Edition
Wording changed only.
Steroids
Level I
- The use of steroids is not recommended for improving outcome or reducing ICP (increases mortality)
Changes from Prior Edition
No changes
Nutrition
Level II A
- Basal caloric replacement at least by the fifth day and, at most, by the seventh day post-injury is recommended to decrease mortality.
Level II B
- Transgastric jejunal feeding is recommended to reduce the incidence of ventilator-associated pneumonia.
Changes from Prior Edition
Emphasised timing and route.
Infection Prophylaxis
Level II A
- Early tracheostomy is when the overall benefit is felt to outweigh the complications associated with such a procedure. (Fewer ventilated days but no less pneumonia).
- The use of povidone-iodine (PI) oral care is not recommended. (No less VAP)
Level III
- Antimicrobial-impregnated catheters may be considered to prevent catheter-related infections during EVD.
Changes from Prior Edition
Removed Periprocedural antibiotics line. Also emphasised VAP is more common in TBI patients.
DVT prophylaxis
Level III
- Low molecular weight heparin (LMWH) or low-dose unfractioned heparin may be used in combination with mechanical prophylaxis. However, there is an increased risk for expansion of intracranial hemorrhage.
- In addition to compression stockings, pharmacologic prophylaxis may be considered if the brain injury is stable and the benefit is considered to outweigh the risk of increased intracranial hemorrhage.
No evidence for specific agent, dose, or timing of pharmacologic prophylaxis.
Changes from Prior Edition
Comment re compression stockings added.
Seizure prophylaxis
Level II A
- Prophylactic use of phenytoin or valproate is not recommended (re late (>7 day) PTS).
- Phenytoin is recommended to decrease the incidence of early PTS, when the overall benefit is felt to outweigh the complications associated with such treatment. NB early PTS have not been associated with worse outcomes.
- No evidence for levetiracetam over phenytoin.
Changes from Prior Edition
No change.
ICP monitoring
Level II B
- Management of severe TBI patients using information from ICP monitoring is recommended to reduce in-hospital and 2-week post-injury mortality.
Old recommendations not carried forward (weak evidence) but re-stated them:
- Intracranial pressure (ICP) should be monitored in all salvageable patients with a severe traumatic brain injury (TBI) (GCS 3-8 after resuscitation) and an abnormal CT. An abnormal CT (hematomas, contusions, swelling, herniation, or compressed basal cisterns).
- ICP monitoring is indicated in patients with severe TBI with a normal CT an 2 or more of:
- age over 40 years
- unilateral or bilateral motor posturing
- systolic blood pressure (BP) <90 mm Hg.
Cerebral perfusion pressure monitoring
Level II B
- Management of severe TBI patients using guidelines-based recommendations for CPP monitoring is recommended to decrease 2-week mortality.
Changes from prior edition
Separated threshold recommendations into different section.
Advanced cerebral monitoring
Level III
- Jugular bulb monitoring of arteriovenous oxygen content difference (AVDO2), as a
source of information for management decisions, may be considered to reduce mortality
and improve outcomes at 3 and 6 months post-injury.
Changes from Prior Edition
Removed brain tissue oxygenation rcommendation removed due to conflicting evidence.
Thresholds
BP
Level III
- Maintaining SBP at ≥100 mm Hg for patients 50 to 69 years old or at ≥110 mm Hg or above for patients 15 to 49 or over 70 years old may be considered to decrease mortality and improve outcomes.
Changes from Prior Edition
New evidence has refined the recommendation.
ICP
Level II B
- Treating ICP above 22 mm Hg is recommended because values above this level are associated with increased mortality.
Level III
- A combination of ICP values and clinical and brain CT findings may be used to make management decisions.
NB RESCUEicp released soon after Guidelines formed.
Changes from Prior Edition
Updated after new study.
CPP
Level II B
- The recommended target CPP for survival and favourable outcomes is between 60 and 70 mm Hg. Whether 60 or 70 mm Hg is unclear, decide for each patient.
Level III
- Avoiding aggressive attempts to maintain CPP above 70 mm Hg with fluids and pressor may be considered because of the risk of adult respiratory failure.
Changes from Prior Edition
Refined after several studies.
Advanced cerebral monitoring
Level III
- Jugular venous saturation of <50% may be a threshold to avoid in order to reduce mortality and improve outcomes.
Changes from Prior Edition
Removed recommendation re brain tissue oxygen monitoring.