
Sepsis remains a syndrome without a validated criterion or standard diagnostic test but increasingly comprehensive data sets are making it easier to test validity of potential criteria. The current instalment of this work in progress has refined the definition of sepsis in light of recent analyses and opinion.
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection
In more detail, sepsis is ‘a multifaceted host response to an infecting pathogen’. It may be significantly amplified by endogenous factors and it involves early activation of both pro and anti-inflammatory responses and major modifications in non-immunologic pathways such as cardiovascular, neuronal, autonomic, hormonal, bio-energetic, metabolic, and coagulation.
Unhelpful truths
- It’s clear that organ dysfunction, even when severe, is not associated with substantial cell death.
- Patients with sepsis are in clinically very heterogeneous groups (age, co-morbidities, injuries, medicines etc.).
- Sepsis-related organ dysfunction may be occult AND unrecognised infection may be the cause of new organ dysfunction.
 “Operationalization”
“Operationalization”
Current definitions have had problems with practical applicability in clinical situations. For example, at least 12% of septic patients don’t have SIRS criteria. And many non-septic patients tick the SIRS boxes.
Are you comfortable with SOFA?
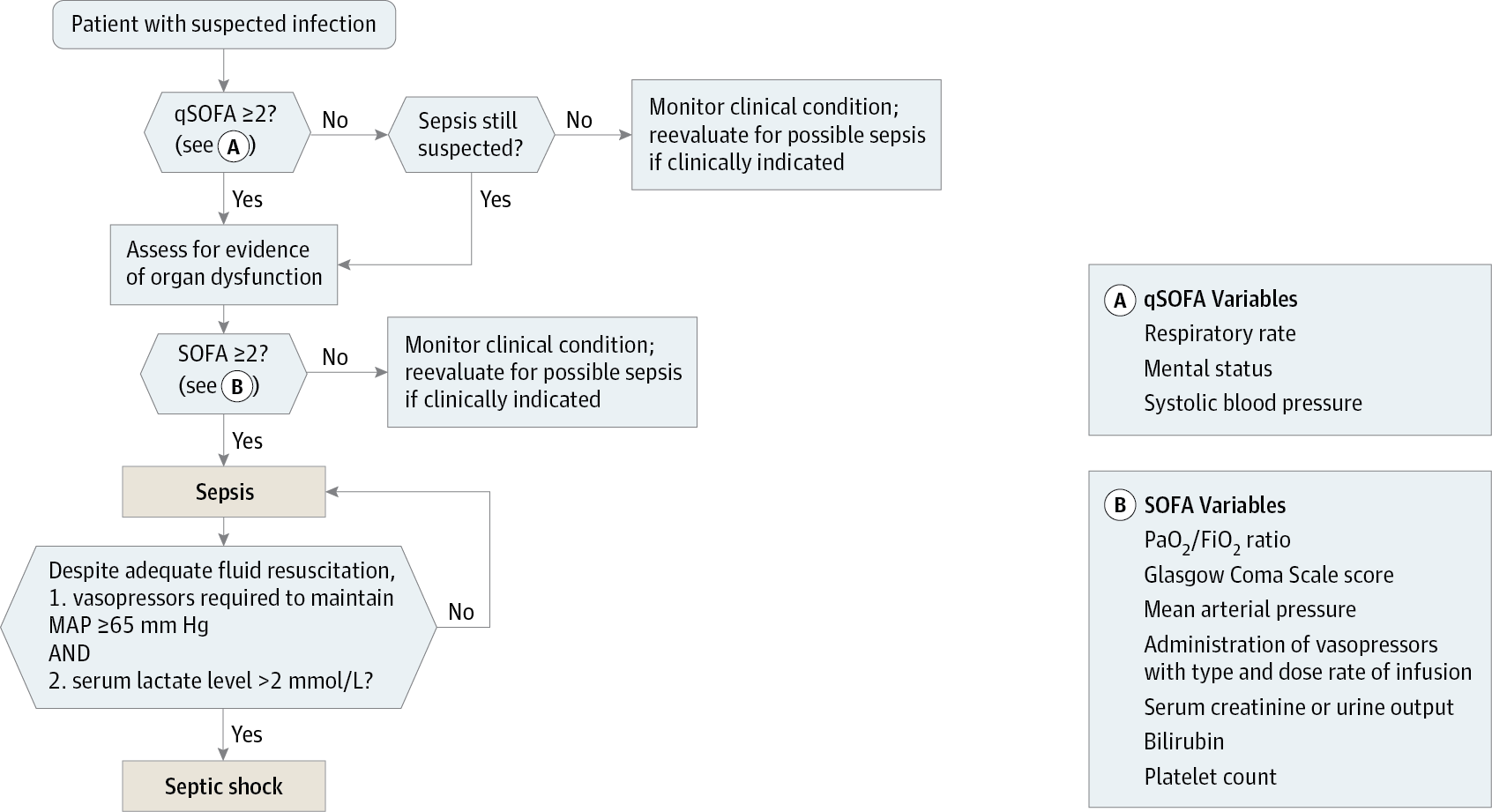
Organ dysfunction is, now, an acute change in total SOFA score of 2 or more points, due to the infection. Assume baseline SOFA of zero, unless you know otherwise. In the presence of infection a SOFA of 2 or more is associated with a mortality rate of 10%.

Further extensive multivariable regression of studies has led to the formulation of the quickSOFA score (qSOFA). Just three parameters can be used to identify patients who are at risk of long stays or ICU death.
A high risk patient has 2 of:
- GCS 13 or less
- Systolic BP < 100
- Respiratory rate > 22
Subgroups of sepsis
Septic shock has been “a state of acute circulatory failure” for many years now despite acknowledgement that this definition is too confined.
This consensus specifies septic shock as sepsis with underlying circulatory and cellular/metabolic abnormalities profound enough to substantially increase mortality (>40%). More pragmatically:
Persisting hypotension requiring vasopressors to maintain MAP > 65 and
serum lactate >2 mmol/L
despite adequate volume resuscitation
Severe sepsis is now felt not to be a useful term.
In summary
- Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection
- We continue to be suspect infection in the normal ways; rash, consolidation, peritonitis, dysuria etc.
- We will continue to wait for dysregulated host responses to be manifest as organ dysfunction.
- SOFA and qSOFA scoring offer a tested means of risk assessing
So what do we do now with the literature on sepsis? Does it all need to be redone or re-analysed?
In addition, this provides more impetus for the development of integrated patient monitoring and information systems. Automated SOFA scoring is surely the corollary of this work, but remains a distant prospect for many hospitals.
All the 2s?
Beware:
- SOFA: decline by 2
- qSOFA: 2 off your GCS, resps of 22, and 2 figure SBP. Any 2 of these.
If it goes unnoticed, you might be calling 2222!
Comment elsewhere
EMCrit/PulmCCM sobering analysis of the new consensus definitions