
Around a third of the mortality from trauma is due to exsanguination. Haemostatic resuscitation, together with permissive hypotension and damage control surgery, is key in severe trauma management and is now very much in focus.
Years of military observational studies (eg here, here, here and there) and expert opinion have suggested that whole blood provides superior resuscitation in the acidotic, hypothermic, coagulopathic trauma patient. In the prospective observational PROMMTT trial, higher ratios of plasma:cells were associated with less early death.
Last month JAMA published PROPPR, a pragmatic USA multisite (level 1 TCs) RCT, involved about 650 patients (with sensible exclusions) who were:
1. ‘highest level trauma activation‘
SBP <90 mmHg,
respiratory compromise,
already needing blood,
abdomen/neck/chest gunshot wounds,
GCS <8,
or otherwise considered severe!
2. taken directly directly from scene
3. received at least 1 unit of blood in the first hour
4. had an Assessment of Blood Consumption score of 2 or more:
1 point for:
penetrating injury,
positive FAST scan,
arrival SBP 90 mm Hg or less,
arrival HR > or = 120.
They were treated with either a 1:1:1 (plasma:platelet:RBC – theoretically equivalent to whole blood) or 1:1:2 transfusion strategy.
Mortality at 24hr and 30 days was not technica lly different between the groups (except briefly at the 3 hour mark interestingly). Overall, the median RBC transfusion was less than 10 units in 24hr, one of the (useless?) definitions of massive transfusion.
lly different between the groups (except briefly at the 3 hour mark interestingly). Overall, the median RBC transfusion was less than 10 units in 24hr, one of the (useless?) definitions of massive transfusion.
Patients in the treatment arm received more platelets and plasma, achieved haemostasis quicker and died less of exsanguination. Cryoprecipitate was barely used at all in this study, and the juries out on how this product fits into haemostatic resuscitation.
One potential criticism is that the treatment arms received platelets immediately whereas the 1:1:2 group received 9 other units of product (3 plasma, 6 RBC) before any platelets. This may have been done to minimise survivor bias (re RBC ratio) but it’s hard to believe this is completely insignificant. Also worth noting that only two thirds got tranexamic acid (given according to elastograms LY-30 etc) but use was similar in each group.
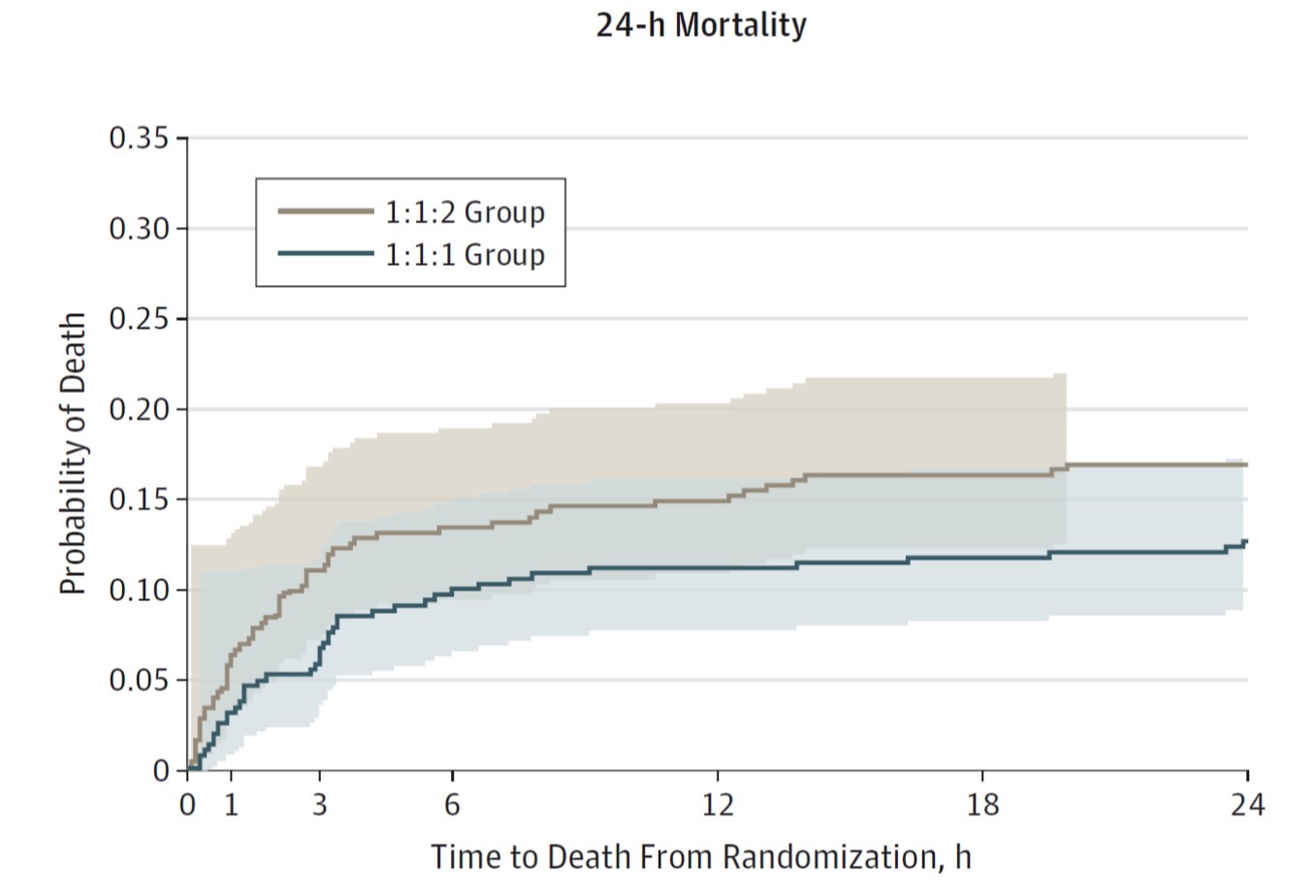
- If the study had been powered to detect a less than 10% difference the result might have been more decisive. Although, strictly speaking, this trial does not show statistical benefit of 1:1:1 over 1:1:2 the Kaplan Meier curve is impressive and with a p value of 0.12 I’m at least 88% sure I’d like to have been in the treatment arm. We can’t be sure 1:1:>2 isn’t safe or better but is seems unlikely and equipoise lack would prevent investigation.
- Strikingly little crystalloid was used – consensus is mounting that blood should be replaced with blood products only.
- If the trend to benefit of the ‘whole blood’ approach is real it probably, as you’d expect, occurs in the first few hours.
- The definition of massive transfusion needs formalizing and time-frame reduced to eg 1-3 hours.
- Could we be less prescriptive and decide dosing dynamically, and is thrombo-elastography ready for this role (because standard coag studies are not practical or useful)?
Some of the best comment:
EMCrit podcast and paper